
In the realm of neurosurgery practice management, there is nothing more central than an efficiently run and well-organized clinic. Developing a shared consciousness regarding patient care and the patient experience with your practice management team that develops into a predictable framework, transforms the clinical experience into a more meaningful one for the patient and more rewarding for the staff and clinician. In this article, I present one clinician’s approach to providing a structure that optimizes efficiencies and the patient experience within each rung of the clinical day. It was a little league baseball game and cervical myelopathy patient that served as my teaching moment and the basis for this article.
One clinic day, early in my career, I was trying to sneak in rounds before beginning my afternoon clinic. My son was the starting pitcher for his baseball team, and I wanted to be at the game from the very start. A new patient was scheduled at the urgent request of a primary physician right before the end of the morning clinic. but with a quick glance of my watch, I noted that I was not too far behind. I felt confident I could quickly see the patient, make a diagnosis, offer a plan of care and still maneuver my way to the hospital and make rounds. In the afternoon, I would be able to leave for my son’s game immediately after seeing my last patient.
In my peripheral vision, I caught a glimpse of the patient I would be seeing walking in with an unbalanced gait, using a cane in one hand and her husband holding the other as my staff roomed them. I became immediately concerned. When I pulled up the images, I sighed in resignation (Figure 1ab). The patient was a 69-year-old woman with profound myelopathy who, according to the notes I had been reviewing, had been given the initial diagnosis of normal pressure hydrocephalus prior to an MRI of the cervical spine. Looking at the scan, I knew the cause of her decline. The signal change on the spinal cord, the multiple levels of stenosis, the profound spondylosis spoke a familiar tale that I would need to explain patiently to the patient and her husband.
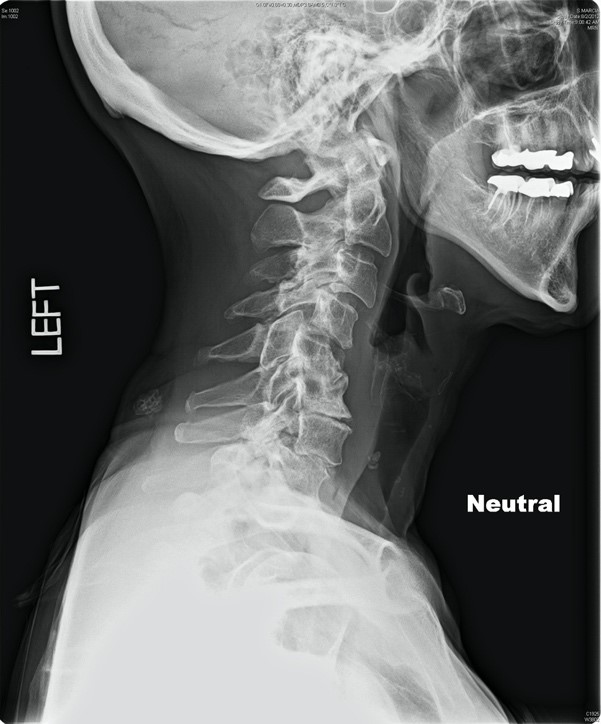
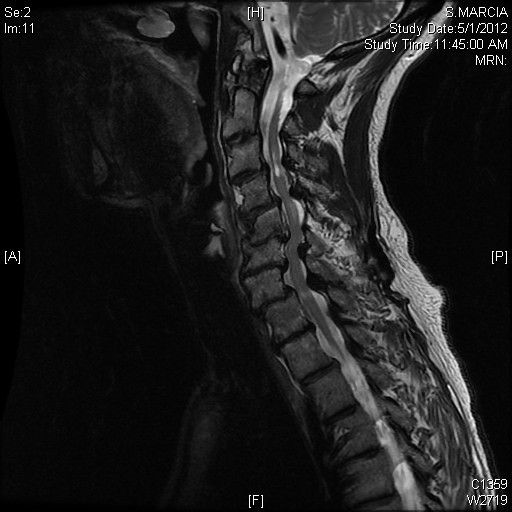
Figure 1ab. Cervical myelopathy. 1a. Lateral radiograph demonstrating profound spondylosis. 1b. Sagittal T2 weighted MRI of a patient who presents with profound cervical myelopathy who had been initially diagnosed with NPH. A patient with cervical myelopathy who needs to understand their diagnosis and treatment will need more time than what is arbitrarily designated for a new patient.
I spent the next hour discussing the natural history of cervical spondylosis with myelopathy, the urgent need for decompression, the complexity of an anterior and posterior operation. Needless to say, I was unable to leave the clinic, much less round over at the hospital before the afternoon clinic would start. By the time I finished the consultation, my team had roomed the first patient of the afternoon and I was already 15 minutes behind. To add insult to injury, I did not make it in time to my son’s baseball game. Instead, my wife sent me short video clips of my little lefty pitching the first few innings. I watched the footage on my phone as I finished hospital rounds over at the hospital and finally made it to see the last half inning of the game.
The two valuable lessons learned from that experience is that even though a new patient slot is designated for 30 minutes, not all new patients have a condition that will fit into that time period. For instance, a patient with a large disc herniation and incapacitating radicular leg pain and dorsiflexion weakness, who has already had an exhaustive course of nonoperative measures may not require much more than 15 minutes to examine and discuss the risks and benefits of a surgery that the patient is clearly ready to undergo. The 69-year-old patient described above is on the opposite end of the patient spectrum. Fifteen minutes just gets the conversation started. The second lesson is the timing of the new patient visit. Should a complex patient be seen at the end of a clinic or at the beginning? The question is, of course, rhetorical.
The solution to the problem begins with organizing a clinic that begins with new patients, then transitions to follow up patients and ends with postoperative patients. A simple half day structure to that clinic would be to begin with three 30-minute new patient time slots, followed by three or four 20-minute follow up time slots and finally end with four or five 15-minute postoperative time slots. The process repeats in the afternoon (Table 1).
New Patient Block |
Three 30 minute slots (1.5 hours) |
Follow Up Block |
Three to four 20 minute slots (1.5 hours) |
Postoperative Evaluations |
Four to five 15 minute slots (1 hour) |
Table 1. A proposed framework for a half day in clinic. Three blocks divided distinctly into new patient, established patient and post-operative patients. The block is repeated in the afternoon in a full day of clinic.
The value to such a structure is that a consistent framework allows your practice management team to work in patients according to their designator, i.e. new patient complex, new patient straightforward, follow up patient straight forward, etc. When a new patient needs to be urgently worked in, your staff will intuitively know when to bring them in and where to put them (Figure 2).
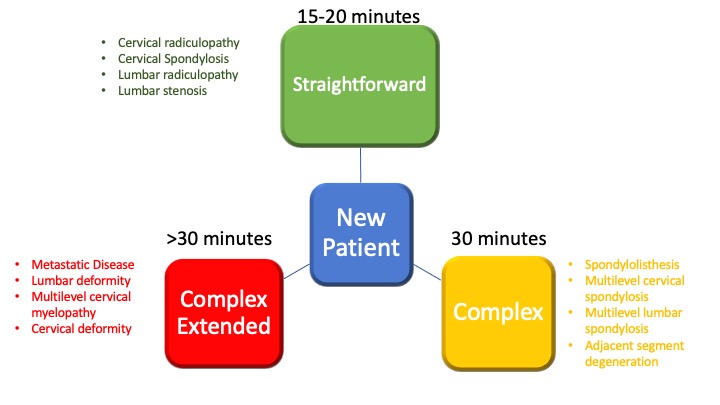
Figure 2. Not all new patients require the same amount of time. Stratifying new patients into these three categories for your staff will help in scheduling patients in a manner that will optimize the flow of clinic.
The second lesson learned from the case above is the complexity of a patient. One look at the sagittal MRI above is all that we need to know that we will need to invest more time into that particular clinical consultation. Couple that with an early diagnosis of normal pressure hydrocephalus and no neck pain, all of a sudden you have the predictable need for additional time. If there are two other straight forward patients before or after, there will be little disruption to the clinical day. If all three new patient visits have the same level of complexity, the entire clinic day will be derailed. The patient experience become compromised, clinical staff and the clinician will be on the receiving end of pent-up frustration because of wait times.
To prevent such a circumstance, a reliable review process, especially for urgent patients, will make you and your staff aware for the potential need for additional time (Figure 2). Access to DICOM cloud-based imaging systems is now ubiquitous. It takes very little investment in time to identify those complex patients, communicate their designators to your staff and make the necessary time for them into your clinical day.
Having your entire practice management team aware of these various clinical circumstances, both the complex and the straightforward, allows them to participate in optimizing clinical efficiencies and the patient experience. The return on that investment pays immediate dividends with a consistent and efficiently run clinic, optimized patient experience and perhaps even providing you the ability to watch your son strike out an opposing batter. I have found that of those experiences carry greater value with every year that passes.

Dr. Tumialán is a neurosurgeon at Barrow Brain and Spine in Phoenix, Arizona. He is the Director of Minimally Invasive Spinal Surgery for the HonorHealth System. He is board certified by the American Board of Neurological Surgery. His expertise includes minimally invasive spine surgery and cervical and lumbar arthroplasty.


