
The 2023 Medicare Physicians’ Fee Schedule brought closure to seven years of advocacy efforts led by the American Association of Neurological Surgeons (AANS), the Congress of Neurological Surgeons (CNS) and the AANS/CNS Section on Disorders of the Spine and Peripheral Nerves (DSPN), in conjunction with other spine societies. These efforts were dedicated to restoring the appropriate valuation of physician work when decompression is performed at the same level as an interbody fusion in the lumbar spine.
In cases where an interbody fusion is performed in the lumbar spine, the bony removal necessary to access the disc space and complete the interbody arthrodesis is included in the interbody fusion codes (CPT® codes 22630 and 22633). However, when patients present with lumbar stenosis causing neurogenic claudication, additional bony work and neural element decompression are required (i.e., decompression on the contralateral side of the spinal canal) to achieve the objectives of the operation. This additional bone work and decompression involve both additional time and risk, and thus, it is crucial to capture the physician’s work through additional codes.
A Bit of History
Before January 2015, additional decompression of the neural elements could be reported with the lumbar laminectomy code (63047) with an appropriate modifier. However, this reporting was restricted after a National Correct Coding Initiative (NCCI) edit published on Jan. 1, 2015. This edit resulted in the ability to capture the additional physician work performed when a decompression was combined with an interbody fusion. Ultimately, the NCCI edit produced a de facto bundling of interbody fusion and lumbar decompression. The details of this process have been previously published.1
Potential solutions were explored, including using the additional level laminectomy code (+63048). Per CPT® coding, +64048 can only be reported with 63047 to describe an additional level of lumbar decompression. No add-on code can be used in isolation, and hospital compliance departments and private payers refused to bill or pay for 63048 in these cases. While championed by another spine society, using +63048 was not an appropriate or viable solution.
New Codes are Developed and Favorably Valued
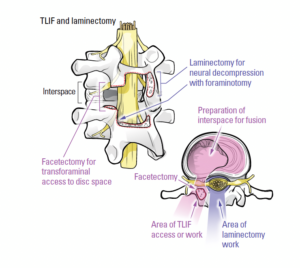
In response to the NCCI and Center for Medicare & Medicaid Services (CMS) recommendations, leading neurosurgery advocates from the AANS, CNS and DSPN developed a new set of codes specific to decompression when performed concurrently with an interbody fusion (63052 and 63053). Representatives from the AANS/CNS Coding and Reimbursement Committee curated the artwork included in the 2022 CPT manual that visually reinforced the argument of the separate and distinct work performed for accessing the interbody space versus decompression of the neural elements. (Figure 1) These codes were developed with other spine societies and valued through the American Medical Association (AMA)/Specialty Society RVS Update Committee (RUC) process and became available for use by spine surgeons on Jan. 1, 2022.
However, this was not the end of the story. In reviewing the new decompression codes, the RUC requested that the interbody fusion codes also be re-surveyed and re-valued. These surveys were completed, and the codes were reviewed at the RUC in April 2021. The total time required to complete the interbody fusion procedures, as described by the new survey results, decreased. However, neurosurgery’s coding and reimbursement experts did not believe this represented a decrease in physician work or a reduction in the complexity of these procedures. Instead, they concluded that the decrease in time was due to streamlining some aspects of the procedure, including using fluoroscopy instead of plain films, electric drills, etc.
Since the times for these procedures had not been assessed in over 10 years, it was not surprising that they decreased due to improved operating room efficiencies and the elimination of inefficient aspects of the operative techniques. The key portions of the procedures and the complexity of treating these patients were not felt to be different. The RUC agreed and recommended very minor decreases in the valuation of the interbody fusion codes, preserving their value.
CMS Disagreed with the Proposed Values and Neurosurgery Springs into Action
CMS disagreed with this recommendation and did not follow the valuations suggested by the AMA and the RUC. In the proposed 2023 Medicare Physician Fee Schedule, CMS offered a substantial further ~10 percent reduction in the valuation of the interbody fusion codes, ignoring the recommendations of the RUC and the deliberations of this expert panel of physicians. This decrease, if finalized, would have significantly undervalued physician work.
Working in conjunction with the International Society of the Advancement of Spine Surgery and other partners, the AANS, CNS and the DSPN sprang into action, organizing a call with CMS leaders, appealing the valuation of lumbar interbody fusion (22630 and 22633) and concurrent interbody fusion and decompression (63052 and 63053) codes. AANS/CNS Washington Office staff, Catherine Jeakle Hill, arranged the meeting, and neurosurgery’s Coding and Reimbursement Committee leaders developed the meeting materials (Joseph S. Cheng, MD, FAANS; John K. Ratliff, MD, FAANS; Luis M. Tumialán, MD, FAANS and others) and led the discussions with CMS (Dr. Ratliff). The call was exceedingly instrumental in improving the value of these codes; this will benefit all spine surgeons.
CMS Reverses Course and Agrees with Neurosurgery’s Recommendations
CMS listened to our concerns and agreed with our position, revising the valuation of the interbody fusion codes in the final physician fee schedule to reflect the recommendations of the RUC, preserving the value of the interbody fusion family, and allowing for appropriate reporting of physician work. CMS’ reversal of the valuation of these codes was a tremendous victory for spine surgeons and spine surgery patients, ensuring Medicare patients’ continued access to medically necessary spine surgery procedures.
Through due process and the advocacy efforts of organized neurosurgery, spine surgeons can once again receive appropriate valuation for decompression performed at the same level as a lumbar interbody fusion thus ending the seven-year saga unraveling the de facto coding bundle.
References
- Tumialán LM, Ratliff JK, Cheng J. Commentary: The Anatomy of Disvalued Codes: The 63047 and the 22633. Neurosurgery. 2019 Feb 1;84(2):E122-E126. doi: 10.1093/neuros/nyy535. PMID: 30649486.
- Saiz P. Lumbar laminectomy code review. SpineLine. July 2014;29-31.

John Ratliff, MD, FACS, FAANS, is program director and professor of neurosurgery at Stanford University. He is immediate past-chair of the AANS/CNS Washington Committee and has served as an advisor to the AMA RBRVS Update Committee for more than 10 years.
Dr. Tumialán is a neurosurgeon at Barrow Brain and Spine in Phoenix, Arizona. He is the Director of Minimally Invasive Spinal Surgery for the HonorHealth System. He is board certified by the American Board of Neurological Surgery. His expertise includes minimally invasive spine surgery and cervical and lumbar arthroplasty.

Katie O. Orrico, Esq., serves as the AANS CEO and has represented organized neurosurgery for 40 years.



