
Imagine a patient is scheduled for surgery, but the insurance company denied the claim. They require a physician-to-physician peer review to discuss appropriateness of the proposed surgery, even with all of the requested items submitted. While waiting for approval, the patient continues suffering from intractable pain with risk for potential neurological deterioration. Sometimes the surgery is approved, but the hospital admission is denied. Neurosurgeons encounter these frustrating scenarios with increasing frequency as the regulatory climate intensifies. But what is the cause?
Managed Care
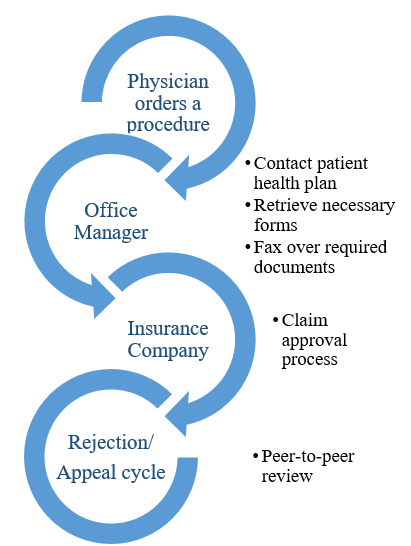
Managed Care allows healthcare plans to regulate spending for non-emergent care. It was popularized in the 1980s to try and subdue the rapidly inflating medical costs for patients.(5,7) Managed Care Organizations (MCOs) try to minimize costs and healthcare utilization, while maximizing the efficiency of care delivery. Prior Authorization (PA) is an administrative process implemented by MCOs to mandate pre-approval for tests, procedures or hospital stays (Figure 1). PA is required by many health plans prior to elective or complex procedures and serves to control costs.(1) Advantage Medicare and Medicaid plans derive from contracts with MCOs that provide a fixed monthly payment per patient. As healthcare is a market-based economy, changes in legislation can impact the net revenue of insurance companies. Thus, in this market-based economy, changes in legislation influence the net revenue of insurance companies, who work off of profit margins.(2,3) The danger in this mixed-economic system is borne by the neurosurgical patient, who needs timely medical care.

For physicians, PA presents a significant challenge to everyday practice. Studies indicate that physicians are frustrated with the delays imposed by the current insurance system. One in three physicians have dedicated staff to manage issues related to PA and 28% reported that delays or denials from PA have led to a serious, adverse patient event.(4) A recent study showed that choice of insurance provider was an independent risk for delays. Since most people have private insurance, they are often surprised by these care restrictions.(3) With Advantage Medicaid and Medicare programs moving away from fee-for-service reimbursements and towards managed-care models, PA requirements are likely to broaden.(5)
A Cumbersome Process
- Plan Variability & Multiple Stake-Holders: The U.S. has no standard for plan provisions outside of those through the exchange. This is further complicated by each company providing many different plans and even levels within similar plans. In addition, many states have individual prior authorization mandates.(5)
- Lack of Transparency: The criteria for approval and list of necessary documentation are not publicly available and may not be evidence-based.
- Limited Reviewer Qualifications: To minimize cost, insurance companies contract tasks to third party benefit management companies.(6) Initial decision-makers may have considerably less specialty experience than the requesting physician/surgeon.
- Inefficiency: The PA process requires coordination across multiple communication channels (7), the majority of which are done by fax or phone (8). Third-party software and other services have been developed to address the need for electronic PA. Nonetheless, these multiple systems are error prone. For example, automated systems might not be able to find a patient if a submission error is made.
What is Being Done
Many individual neurosurgeons have written about their approaches to prior authorization. The AANS and CNS have applauded lawmakers for asking Centers for Medicare & Medicaid Services (CMS) to review practices.(9) They are continuing to work with the AMA in their PA reform efforts, which urge CMS to issue guidance to healthcare plans on PA.(10)
The Council of State Neurosurgical Societies (CSNS) has designed an integrated care pathway specific to neurosurgical patient populations and practice. A resolution adopted this year encourages the AANS and CNS to work with the AMA to advocate for legislation requiring MCOs to institute transparent and accountable processes for peer-to-peer review in neurosurgery.
Relevancy to Medical Students
Medical education is a translational process, where we gain both the knowledge to provide healthcare for patients while functioning within the complex medical system. Medical schools recognize the need to provide crucial education beyond the medical sciences with integration of bioethics, humanities, and communication skills as examples. Still an increasing number of students seek out secondary degrees in public health and business (e.g. MPH, MBA, MPA).(11) Consequentially, we should advocate for the integration of these material into the current curriculums. It is imperative that young neurosurgeons be familiarized with issues in the field and trained in the skills to deal with them.
Healthcare is a network of interconnected components, each with a unique role and function through processes that aim to improve the care of patients. A defect in a link is felt by the entire network. PA was created to restrict access to what insurance companies deem as costly services and provide affordable quality care.(1) However, restricting access in neurosurgery can have insurmountable and fatal consequences.
References
1. Harrington, M. K. (2015). Health care finance and the mechanics of insurance and reimbursement. Burlington, MA: Jones & Bartlett Learning.
2. Medicaid Managed Care Quality. (n.d.). Retrieved from https://www.medicaid.gov/medicaid/quality-of-care/medicaid-managed-care/index.html
3. Menger, R. P., Thakur, J. D., Jain, G., & Nanda, A. (2017). Impact of insurance precertification on neurosurgery practice and health care delivery. Journal of Neurosurgery, 127(2), 332-337.
4. AMA. (2019). 2018 AMA Prior Authorization Physician Survey. Retrieved from https://www.ama-assn.org/system/files/2019-02/prior-auth-2018.pdf
5. AMA. (2019). Prior authorization: The current landscape. (p. 4). Retrieved from https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/premium/psa/prior-authorization-toolkit_0.pdf
6. Davis, E. (2018, November 25). How to Get a Pre-Authorization Request Approved by Your Health Plan. Retrieved from https://www.verywellhealth.com/how-to-get-a-prior-authorization-request-approved-1739073
7. Colligan, L., Sinsky, C., Goeders, L., Schmidt-Bowman, M. & Tutty M. (2016). Sources of physician satisfaction and dissatisfaction and review of administrative tasks in ambulatory practice: A qualitative analysis of physician and staff interviews. Retrieved from https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/ps2/ps2-dartmouth-study-111016.pdf
8. AMA. (2019). Measuring progress in improving prior authorization. Retrieved from https://www.ama-assn.org/system/files/2019-03/prior-auth-survey.pdf
9. CSNS. (2018). Neurosurgeons Applaud Lawmakers for Asking CMS to Review Prior Authorization Practices. Retrieved from https://www.cns.org/sites/default/files/legislative/neurosurgeons_commend_lawmakers_for_supporting_review_of_prior_auth_fina.pdf
10. AANS. (2019). AANS and CNS Urge CMS to Issue Guidance to MA Plans on Prior Authorization. Retrieved from https://www.aans.org/en/DC-E-News/2019/May-2019/AANS-and-CNS-Urge-CMS-to-Issue-Guidance-to-MA-Plans-on-Prior-Authorization
11. Viswanathan, V. (2018, March 30). The Rise of the M.D./M.B.A. Degree. Retrieved from https://www.theatlantic.com/education/archive/2014/09/the-rise-of-the-mdmba-degree/380683




