
The views expressed in this article are those of the author(s) and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense or the U.S. Government.
The decade of the 1940s started with a world at war. World War II (WWII) began in 1939, and American involvement began two years later. Almost every facet of life was touched by the war, and neurosurgery was no exception. Many of the advances in the field during the first half of the decade were directly related to the treatment of wartime casualties.

World War I (WWI) had seen extremely high mortality rates for casualties with head and spinal cord injuries. The neurosurgeons who served in WWII dedicated their efforts at strategies to avoid repeating those same high rates. Based on his experience during WWI, Harvey Cushing opined that mortality could be reduced by 50 percent if casualties could receive operative intervention in forward areas of the battlefield (1). Brigadier Sir Hugh Cairns of Great Britain, a former student of Cushing’s at Harvard, who had cared for WWI legend T.E. Lawrence (of Arabia) after his fatal motorcycle accident, built on this supposition, by developing the Mobile Neurosurgical Unit (MNSU). This typically offered forward capability for the treatment of neurosurgical casualties within 48 hours of injury.
MSNUs were staffed with a neurosurgeon, neurologist, anesthetist, two general duty physicians, two Queen Alexandra sisters (nurses with the equivalent rank of Lieutenant in the Queen Alexandra Imperial Military Nursing Service), four orderlies and two drivers. Such units were equipped to perform up to 200 operations. While the first MNSU had an inauspicious start (they were captured), eight more MNSUs were created and seven were actually fielded with exceptional results. Those units were deployed in both the European and Pacific theaters of operation with service in North Africa, Italy, France, India and Asia. Remarkable improvements in the rates of infection (meningitis, brain fungus and abscess) were realized with a drop from approximately 25-5 percent (6). In all, nearly 20,000 casualties were treated at the MNSUs (1,6).
Advancements in Neurosurgery
Important trends that emerged from the treatment of WWII casualties:

- Recognizing the need for early surgery
- Benefits of segregation of head-injured patients into specialized units
- Providing definitive surgery to debride the wound and to remove all but the deepest of in-driven bone and metallic fragments at the initial operation
- Wide use of antiobiotics (Sulfanilamides initially , later penicillin, proved to be very effective)
Primary closure was obtained in nearly 97 percent of cases, and subsequent surgeries were required in such cases only for reconstruction (6).
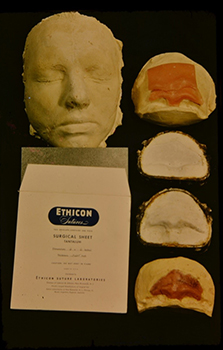
Advances in cranioplasty also emerged as a result of treating wartime casualties (1,7). John C. Neill, MD, a neurosurgeon in Mississippi, shared the experiences of his father, Dr. Charles Neill, who served in World War II at the 1st General Hospital in New Mimms Park, England (Figures 1 and 2 kindly shared). One is an operation report while the other shows the mask and tantalum implant he used. The report explains the process of first making a plaster of Paris mold, using wax to create the model and then using tantalum to form the actual implant.
The treatment of spinal cord injuries also evolved substantially during WWII. While the mortality rate during WWI was extremely high, improvements largely in the peri-operative management of those casualties proved most beneficial (7). The prevention of bedsores, as well as attention to nutrition and careful bladder management, led to meaningful gains in survival. Dr. Lawrence Pool (LtCol, USA, Ret), who served at the 9th Evacuation Hospital, wrote that water-tight dural closure was critical and that laminectomy was the most commonly performed operation of the spine. Over half of his patients demonstrated neurological improvement following surgery (5). While the one-year mortality of paraplegics in WWI was approximately 90 percent; nearly 75 percent of paraplegics from WWII were alive at 20 years (1).
Nerve injuries were also exceedingly prevalent during WWII. In his account of his experience with the 9th Evacuation hospital, Dr. Pool noted that such injuries were not repaired acutely due to the operative resources they consumed; rather, they were treated after subsequent evacuation to general hospitals (5). While at the 1st General Hospital in England, Dr. Neill recorded that approximately 60 percent of his workload consisted of peripheral nerve cases. It was believed that such injuries were ideally treated at three to six weeks status post injury, and because these patients were assigned the lowest triage category for evacuation, they often arrived at the general hospital within that treatment window (personal communication with Dr. John Neill).
Specialization Required
Another important neurosurgical outcome of WWII was the recognition of the need for additional specialized training. Neurosurgeons were in very short supply on the battlefield and, by necessity, many still performed general surgical procedures. In order to prepare general surgeons and partially-trained neurosurgeons for military service, many underwent a four-month (or sometimes longer) training program to better prepare them for the types of patients they would treat.
Dr. Neill has reported that his father acknowledged initially feeling inadequately prepared for the kinds of wounds he would treat due to the fact that he had not been able to attend such a course. However his superiors felt that his six months of neurosurgery as part of his general surgery training were adequate. Despite his self-perceived deficiency, he grew very adept in his skills, in part with experience and in part through the excellent mentorship of Col. R. Glen Spurling and the British neurosurgeon Mr. John O’Connell.
Many surgeons returned from war wanting to expand their formalized neurosurgical training, and several programs were therefore established in the latter part of the 1940s. CAPT (ret) Morris “Bud” Wade Pulliam, MD, FAANS(L), himself a veteran of the Vietnam conflict, shared that military service was highly valued in the neurosurgery community during his training at Washington University’s program under Henry Gerard Schwartz, MD. Dr. Pulliam related that while Dr. Schwartz would not frequently bring up his service, he would speak passionately about his WWII experience in North Africa when asked, and he remained connected to the Army as a senior consultant through the Vietnam era.
Psychosurgery
Other neurosurgical advances in the 1940s centered largely on functional neurosurgery, especially as it related to the treatment of mental disease. Psychosurgery had gained interest in the 1930s, having been considered a reasonable alternative to treating severely affected patients for whom there was no available and effective medical treatment. Though prefrontal lobotomy was an imprecise surgery fraught with the possibility of severe side effects, it had gained substantial use. This advance was a catalyst for work done in the 1940s aimed at minimizing what was dubbed “post-leukotomy syndrome.”
William Beecher Scoville, MD, a neurosurgeon at Hartford Hospital, developed techniques to target specific pathways and disrupt the fiber connections in the medial frontal areas (4). Others of this era were interested more in deep brain lesioning to address psychiatric disorders. This spurred a desire to be able to make reliable lesions in the dorsomedian nucleus of the thalamus to potentially effect behavior with less disability. Then, in 1947, the neurologist Ernest A. Spiegel, MD, and the neurosurgeon Henry T. Wycis, MD, both of Temple University, published their landmark study introducing a stereotactic frame to use for psychiatric illness, pain and movement disorders. They called their procedure stereoencephalotomy. Previously, the Horsley-Clarke frame had been used on animals and relied largely on skull landmarks (2). The strides made in radiography, pneumoencephalography and neurophysiology all converged to allow the development of a stereotactic system that used internal structures for guidance.
Though surgery for psychiatric disease had initially spurred the development of the frame (4), within a year of publication, their groundbreaking advance was already being used to treat patients with Huntington’s chorea. While interest in psychosurgery waned, due to ethical considerations and the development of new medications, interest in treating movement disorders grew and rapid advanced throughout the 1950s (4).
Thus, the neurosurgeons practicing in the 1940s had enormous influence in shaping future neurosurgeons. Neurosurgeons born in the 1940s reaped the benefits of the knowledge and ethos espoused by these prominent pioneers. They not only affected the residents they trained directly, but produced the future chairs that continued these traditions. AANS vice president, Moustapha Abou-Samra, MD, FAANS, spoke of his time as a trainee under Jim L. Story, MD, FAANS(L), at the University of Texas at San Antonio. Interestingly, Dr. Story and Willis E. Brown Jr., MD, FAANS(L), trained under Lyle A. French, MD at the University of Minnesota. Dr. French, a renowned neurosurgeon who himself had served in WWII, had a profound influence on those he taught and, consequently, on the programs in which his trainees eventually served. Likewise, Dr. Pulliam (CAPT, USN, Ret), who was trained by Dr. Schwartz at Washington University, related for many years, Dr. Schwartz had been the faculty member who had trained the most program chairs in the US. Both Drs. Abou-Samra and Pulliam spoke of the incredible work ethic, the intellectual honesty and the complete dedication to the field that these men and their protégés fostered. The atmosphere at their programs was tough and the level of expectation very high. Praise was scant and criticism plentiful, but those hard-fought lessons forged them into the neurosurgeons they are, with exceptional devotion to their patients and dedication to our ever-changing field.
Acknowledgements: I would like to thank AANS members Dr. Abou-Samra, Dr. Morris Pulliam and Dr. John Neill for generously sharing their experiences (and for Dr. Neill’s photos).
Moustapha Abou-Samra, MD, FAANS, is the current vice president of the AANS and past president of the Neurosurgical Society of America. He trained at the University of Texas at San Antonio under Jim L. Story, MD, FAANS(L), and has practiced as a private practice neurosurgeon for 36 years in Ventura, Calif.
Morris Wade “Bud” Pulliam, MD, FAANS(L), trained at Washington University under Henry Schwartz, MD. He served in the U.S. Navy, retiring as a Captain in 1997 and then practiced in Youngstown, Ohio, in private practice until his retirement.
John C. Neill, MD, FAANS, trained in neurosurgery at the University of Mississippi. He had a robust general neurosurgical practice in Jackson, Miss., until he retired from full time practice three years ago. Both Dr. Neill’s father (Dr. Charles Neill) and his father-in-law (Dr. Robert Watson) were neurosurgeons as well.
I am a military service member. This work was prepared as part of my official duties. Title 17 U.S.C. 105 provides that ‘Copyright protection under this title is not available for any work of the United States Government.’ Title 17 U.S.C. 101 defines a United States Government work as a work prepared by a military service member or employee of the United States Government as part of that person’s official duties.
5. Pool, J. L. (2000). Neurosurgical Notes: World War II. Neurosurgery, 46(3), 721-729.
8. Personal communications with Dr. Moustapha Abou-Samra April 2017, Dr. Morris “Bud” Pulliam May 2017, and Dr. John Neill, May 2017.
[aans_authors]




